Ozempic side effects like nausea and stomach discomfort get all the attention — but there’s a far more serious risk quietly affecting a large proportion of GLP-1 users that most doctors aren’t adequately warning about. Ozempic changed everything. Millions of people have lost significant weight on GLP-1 drugs, and the cardiovascular and metabolic benefits are real and well-documented. By almost any measure, these medications represent one of the most significant advances in obesity medicine in decades.
But there’s a risk that’s not getting nearly enough attention — one that quietly affects a large proportion of people on these drugs, that can have serious long-term consequences, and that most patients are never adequately warned about before starting treatment.
It’s not nausea. It’s not the gastrointestinal side effects you’ve probably already heard about.
It’s muscle loss — and the downstream health consequences it sets in motion.
The Problem Nobody Is Talking About Loudly Enough
Here’s the uncomfortable truth about GLP-1 drugs: they don’t discriminate between fat and muscle when they help you lose weight.
Studies consistently show that people on semaglutide and tirzepatide lose a significant proportion of their total weight loss as lean muscle mass — not just fat. Estimates from clinical trial data suggest that anywhere from 25% to 40% of the weight lost on these medications comes from lean tissue rather than fat.
To put that in concrete terms: if someone loses 40 pounds on Ozempic, they may lose 10–16 pounds of that as muscle — not fat.
This isn’t unique to GLP-1 drugs. All significant weight loss — whether from calorie restriction, bariatric surgery, or medication — tends to involve some muscle loss alongside fat loss. But the scale and speed of weight loss on GLP-1 medications, combined with the reduced appetite that makes it harder to eat enough protein, can make the muscle loss problem particularly pronounced.
Why Losing Muscle Is a Much Bigger Deal Than Most People Realize
Muscle loss sounds like a vanity concern — something that affects how toned you look, not your actual health. But that framing seriously undersells how important muscle tissue is to your overall wellbeing.
1. Muscle Loss Slows Your Metabolism — Permanently
Muscle is metabolically expensive tissue. It burns calories at rest, keeps your metabolism running efficiently, and helps regulate blood sugar. When you lose muscle, your resting metabolic rate drops — meaning your body needs fewer calories to maintain its new weight.
This creates a trap: you lose weight, lose muscle in the process, your metabolism slows, and the calorie intake that maintained your new weight now causes you to gain weight again. This is a major driver of the weight regain pattern seen after stopping GLP-1 drugs.
2. Muscle Loss Dramatically Increases Fall and Fracture Risk
This is especially critical for older adults. Muscle strength — particularly in the legs and core — is the primary defense against falls. Falls are the leading cause of injury-related death in adults over 65, and loss of muscle mass is one of the key factors that makes falls more likely.
People who lose significant muscle while on GLP-1 drugs may end up at substantially higher fall risk — which somewhat offsets the cardiovascular and metabolic benefits of the weight loss.
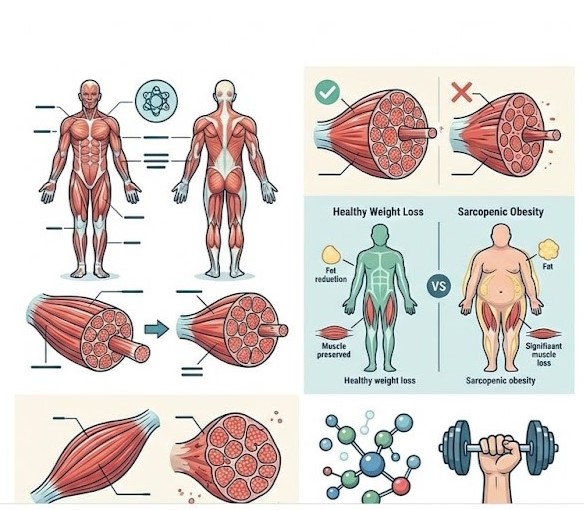
3. Sarcopenic Obesity: The Worst of Both Worlds
There’s a condition called sarcopenic obesity — having both excess body fat and insufficient muscle mass. It’s increasingly recognized as more metabolically dangerous than either condition alone.
Here’s the concern: someone who loses weight on a GLP-1 drug but loses a disproportionate amount of muscle could end up in a better weight category on paper while actually having a worse body composition — more fat relative to muscle — than before treatment began.
4. Functional Decline
Beyond the numbers, muscle loss has a direct impact on daily function. Getting up from a chair. Climbing stairs. Carrying groceries. Opening jars. These everyday tasks become measurably harder as muscle mass declines. For older adults especially, this loss of functional capacity is directly tied to independence and quality of life.
5. Bone Density Reduction
Muscle and bone are closely linked. Muscle contractions during physical activity stimulate bone density. When muscle mass declines, the mechanical stimulus for bone maintenance decreases — contributing to bone loss and elevated fracture risk, particularly in postmenopausal women already at risk for osteoporosis.
Who Is Most at Risk
Not everyone on GLP-1 drugs faces the same level of muscle loss risk. Certain profiles are significantly more vulnerable:
Older adults (65+): Already experiencing natural muscle loss (sarcopenia), older adults have less muscle reserve to lose and face more serious functional consequences when they do.
People who are not exercising during treatment: Physical inactivity is the fastest route to muscle loss during any calorie-restricted period. People who rely on the drug alone without incorporating resistance training lose substantially more muscle than those who train.
People with inadequate protein intake: Reduced appetite — the primary mechanism of GLP-1 drugs — makes it easy to fall short of protein needs. Without sufficient dietary protein, muscle preservation is significantly compromised.
People losing weight very rapidly: Faster weight loss is associated with greater proportional muscle loss. The dramatic weight loss seen with higher doses of semaglutide or tirzepatide amplifies this risk.
People with already low muscle mass: Those starting treatment with below-average muscle mass for their age and size have less room for loss before functional problems emerge.
The 4 Strategies That Protect Your Muscle While on GLP-1 Drugs
The good news: muscle loss on GLP-1 medications is not inevitable. It’s highly modifiable with the right approach.
Strategy 1: Resistance Training — Non-Negotiable
This is the single most important thing you can do. Resistance training — lifting weights, using resistance bands, bodyweight exercises — provides the mechanical stimulus that tells your body to preserve muscle tissue even in a calorie deficit.
Aim for at least 2–3 resistance training sessions per week, targeting all major muscle groups. This doesn’t need to be intense or complicated — a simple full-body routine is sufficient.
Research shows that people who combine GLP-1 medication with regular resistance training lose significantly more fat and significantly less muscle than those who don’t train.
Strategy 2: Hit Your Protein Targets
Protein is the building block of muscle. During weight loss — especially rapid weight loss — protein requirements actually increase because the body needs more amino acids to preserve lean tissue.
The recommended target for people on GLP-1 drugs is at least 1.2–1.6 grams of protein per kilogram of body weight per day — significantly higher than the general population recommendation.
Given that GLP-1 drugs reduce appetite, hitting these protein targets requires intentionality. Prioritize protein at every meal — eat it first, before vegetables and carbohydrates, to ensure you hit your targets even when overall food intake is reduced.
Good high-protein options include: eggs, Greek yogurt, cottage cheese, chicken breast, fish, lean beef, tofu, edamame, and protein shakes when needed.
Strategy 3: Don’t Cut Calories Too Aggressively
Extremely aggressive calorie restriction amplifies muscle loss. While GLP-1 drugs naturally reduce calorie intake, try to avoid going below 1,200–1,400 calories per day (for women) or 1,500–1,600 calories per day (for men) without medical supervision.
Slower, more gradual weight loss — even if it feels less satisfying in the short term — preserves more muscle and produces better long-term body composition outcomes.
Strategy 4: Consider Creatine Supplementation
Creatine monohydrate is one of the most well-researched supplements in existence, with a strong safety profile and consistent evidence for supporting muscle mass and strength during periods of calorie restriction.
A dose of 3–5 grams per day is the standard recommendation. It’s inexpensive, widely available, and may help offset some of the muscle loss associated with GLP-1 drug use. Discuss with your doctor before adding any supplement to your regimen.
What to Ask Your Doctor Before Starting GLP-1 Treatment
If you’re considering or currently on a GLP-1 medication, here are 5 questions worth raising with your physician:
- “What can I do to minimize muscle loss while on this medication?”
- “Should I have a baseline DEXA scan to measure my body composition before starting?”
- “What protein intake should I be targeting?”
- “Should I be working with a dietitian or exercise physiologist during treatment?”
- “How will we monitor my muscle mass and bone density over time?”
These questions reflect a more complete picture of GLP-1 drug management than many patients currently receive — and asking them signals to your doctor that you want a comprehensive approach, not just a prescription.
Frequently Asked Questions (FAQ)
Q: How much muscle can you lose on Ozempic? A: Studies suggest that 25–40% of total weight lost on GLP-1 medications may come from lean muscle mass rather than fat. The exact amount varies based on exercise habits, protein intake, age, and the rate of weight loss.
Q: Can you prevent muscle loss on Ozempic entirely? A: You can’t prevent it entirely during significant weight loss, but you can dramatically reduce it. People who do regular resistance training and hit adequate protein targets lose substantially less muscle — and more fat — than those who don’t.
Q: Does muscle loss from Ozempic come back after stopping? A: It can, but it requires deliberate effort — specifically, resistance training and adequate protein intake. Muscle loss doesn’t automatically reverse when you stop the medication. You have to actively rebuild it.
Q: Is muscle loss from GLP-1 drugs worse than from regular dieting? A: Potentially, yes — because GLP-1 drugs can produce more rapid and significant weight loss than traditional dieting, and faster weight loss is generally associated with greater proportional muscle loss. The reduced appetite also makes it harder to maintain adequate protein intake.
Q: Should everyone on GLP-1 drugs do resistance training? A: Based on current evidence, yes — for virtually all patients. The muscle preservation benefits of resistance training during GLP-1 treatment are well-documented and significant enough that most obesity medicine specialists now recommend it as a standard part of treatment.
Q: Are newer GLP-1 drugs better for preserving muscle? A: This is an active area of research. Some newer dual and triple agonist medications in development appear to have more favorable effects on body composition. Tirzepatide (Mounjaro/Zepbound) may have slightly better muscle preservation profiles than semaglutide, though research is ongoing.
The Bottom Line
GLP-1 drugs are genuinely remarkable medications — but the muscle loss risk is real, it’s significant, and it’s not being communicated loudly enough to patients.
Losing 25–40% of your weight loss as muscle isn’t a minor side effect. It affects your metabolism, your fall risk, your functional capacity, your bone density, and your long-term ability to maintain your results. For older adults especially, this risk deserves serious attention.
The solution isn’t to avoid these medications — for the right patients, the benefits far outweigh the risks. The solution is to take the muscle loss risk seriously from day 1, combine medication with resistance training, prioritize protein, and work with a healthcare team that monitors body composition — not just body weight.
Weight on the scale tells only part of the story. What you’re made of matters just as much as how much you weigh.